As mentioned in the 1st SMARTsurg newsletter, we have chosen a total of seven use cases on urology, cardiovascular and orthopaedic surgery. The surgical workflow of these surgical use cases is represented in a graphical format with the components of the surgical activity, for example, “Phases” of the surgery.
To obtain user-specific requirements in minimally invasive robotic surgery, a total of 29 surgeons, of urology, orthopaedic and cardiovascular specialties, are interviewed as shown in the following table:
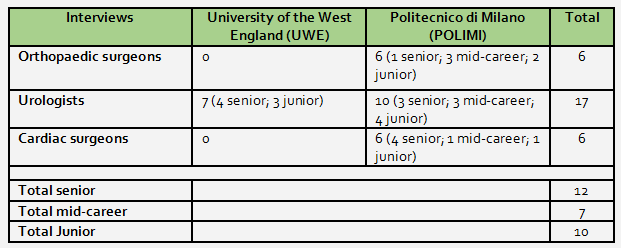
We used a set questionnaire to conduct the interviews, whereby two types of questions have been considered. Surgeon’s expressed their opinions in the expressive form, provided answers in the form of Yes/ No or expressed their answers by selecting one or more options. We organised and structured recorded audio data of the interviews into verbatim transcripts for further analysis. The participating surgeons provided various answers, which were later grouped together against each question of the questionnaire. We analysed data within the specialties (i.e. interview data of orthopaedic surgeons, urologists and cardiac surgeons separately), referred to as the ‘within-case’ analysis. The ‘within-case analysis’ was used to identify common categories or a theme for the user requirements from each surgical use case; e.g. better ‘image quality’, as a defined as a category from urologists. After the ‘within-case’ analysis, we analysed the specialties, i.e. common requirements between different specialties; the ‘across-case’ analysis. During the ‘across-case’ analysis, the identified requirements were prioritised, against a scoring scale of 1 to 5, during the SMARTsurg consortium meeting (Milan, Italy, 10-11 July 2017). Most of the end-users presented and gave their contribution in identifying the priorities. In total we elicited of 33 mandatory user requirements out of which 4 requirements were mandatory:
- superimposed preoperative images,
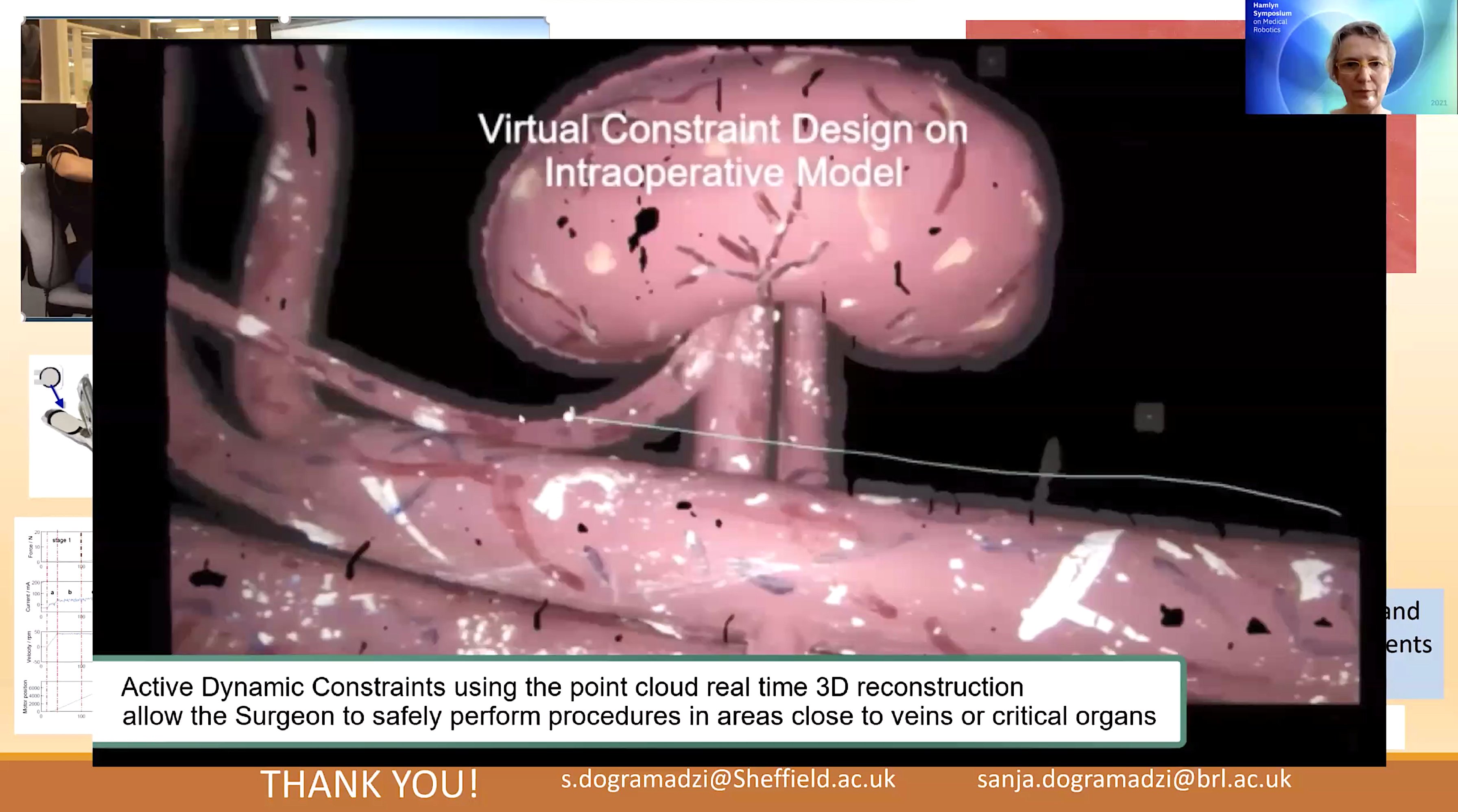
- active constraints (an anatomical region which is defined preoperatively to stop the robot move outside of this region),
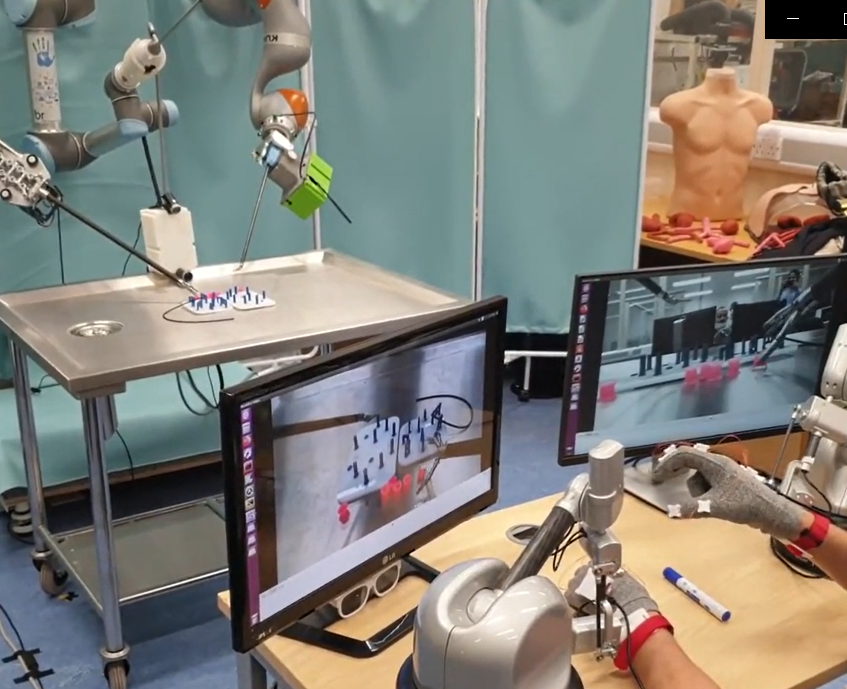
- articulated instruments,
- hand exoskeleton (as surgeon’s side master system).
The elicited requirements have been put in correspondence with the system hardware and clinicians' feedbacks was taken into account when choosing the final application scenarios choice.
SMARTsurg three application scenarios synopsis with user requirements:
1. Robot-assisted Partial Lateral Meniscectomy (RaPLM)
A meniscus tear is a common knee joint injury, RaPLM is performed to remove of all or part of a torn meniscus. Smart glasses (for assistants) a hand exoskeleton, better image quality and articulated instruments are needed in all the phases of RaPLM. In first phase of RaPLM surgeons need to overview the knee joint, where the three-fingered instrument could be used to see the knee compartments. In order to evaluate the position of the tear in the meniscus, which is done conventionally by marking the damage by the probe, however a haptic perception, “a sense of touch”, could prove useful. During the RaPLM, pre-operative images could be superimposed to see the damaged meniscus, enable the surgeon to cut it minimally. Finally, the three-fingered instrument could be used to cut the free cartilage pieces, where active constraints could also be implemented to prevent the injury to the meniscus rim and to cut the minimum meniscus.
2. Robot-assisted Partial Nephrectomy (RAPN)
RAPN is performed to remove tumorous portions of the kidney. A hand exoskeleton, better image quality, smart glasses (for assistants) and 3D images (for visualization) are required in all the phases of RAPN. During the preparation of the kidney, active constraints could be used to prevent the injuries to vasculature such as, the aorta or vena cava as well as, organs such as the liver or spleen. After that, during the excision of the tumour, preoperative images are superimposed to view the renal artery, while incising the renal capsule before clamping the artery. After the preoperative images are superimposed, active constraints could be used to prevent the injury of renal arteries. After that, haptics could be used for the closure of renal breach during suturing and pulling of the thread while doing the suturing of the kidney.
3. Robot-assisted Coronary Artery Bypass Grafting (CABG)
CABG is advised in the patients with significant narrowing or blockage of coronary artery. A hand exoskeleton, better image quality, smart glasses (for assistants), and 3D images are required in all the phases of CABG. Firstly, during the LIMA (Left Internal Mammary Artery) phase take down, pre-operative images could be used to identify LIMA and the thymus gland. Then, active constraints could be used for preventing the injuries to LIMA while cauterising the sternal branches or using the diathermy. Before the LIMA takedown, haptics could be used to assess the calcium deposits, if any, in the coronary artery. Articulated instruments could then be used to take down LIMA and reach the posterior side of the heart, e.g. to assess the posterior branch of the coronary artery. During LIMA-LAD (Left Anterior Descending Artery), which is a branch of a coronary artery anastomosis, haptics could be incorporated during suturing and pulling of the thread, where the three-fingered instrument could be used to cut the sutures.